
Olivia M Kimario1*, Fabian Massaga1, Enica Richard 2
1Department of Surgery, Catholic University of Health and Allied sciences p.0.box 1464 Tanzania.
2Department of ORL, Muhimbili University of Health and Allied sciences, p.o.box 65001 Tanzania.
Corresponding Author: Olivia Michael Kimario, Department of otorhinolaryngology, Catholic university of health and allied sciences p.0.box 1464 Tanzania.
Received Date: January 13, 2024
Accepted Date: January 19, 2024
Published Date: January 22, 2024
Citation: Olivia Michael Kimario, Enica Richard and Fabian Massaga. (2024) “Epidemiological Patterns of Pharyngeal Malignancies in Tanzania: A Descriptive Cross-Sectional Study.”, Clinical Case Reports and Clinical Study, 11(1); DOI: 10.61148/2766-8614/JCCRCS/165
Copyright: © 2024 Olivia Michael Kimario. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This manuscript presents a descriptive cross-sectional study conducted at Muhimbili National Hospital in Tanzania, aiming to explore the prevalence, demographic distribution, histological types, and clinical characteristics of pharyngeal malignancies in the region. The study spans from April to December 2015 and includes 438 patients diagnosed with head and neck malignancies, with a specific focus on 114 cases of pharyngeal malignancies. The results provide valuable insights into the age, gender, site, and histological distribution of these malignancies.
Conclusion: The finding of this study shows the prevalence of pharyngeal malignancies among head and neck malignancies was 26% with the leading histological type been Squamous cell carcinoma been the predominant in both sexes.
Introduction:
Head and neck malignancies are types of primary malignancies that occurs in the upper aerodigestive tract or is a group of biologically similar cancers arising in the upper aero-digestive tract, that includes mouth (oral cavity), lip, paranasal sinuses, nasal cavity, larynx, and pharynx [1].
Pharyngeal malignancies includes those of the nasopharynx, oropharynx and hypopharnx. This malignancies has been on the rise due to changes of life style and adaptation of the people to different geographical region.
Pharyngeal malignancies is increasing in its incidence in developing countries mores as compared to developed countries due to social economic status [2]. Nasopharyngeal carcinoma (NPC) one of the type it occur rarely although some parts of the world like south east Asia and some parts of middle east and north Africa it has been reported to have high prevalence. Male been more involved than female in terms of gender.
The incidence of Nasopharyngeal carcinoma tends to increase with increasing age, it has a bimodal pattern of distribution observed with peak incidence in late adolescent and another peak in the fifth or sixth decade of life [3,4].
Oropharyngeal cancer is number sixth in the occurrence of cancer worldwide [5].The prevalence is higher in males than females [6][7]. Oral sex and open-mouthed kissing are the most common reasons for oral HPV infection [5].HPV-associated oropharyngeal squamous cell carcinoma occurs in patients who have been infected with the human papillomavirus. Among the many types of human papillomavirus, HPV16 is the most common type found in oropharyngeal cancers [6]. HPV-associated OPSCC tends to occur in a younger population that smokes and drinks less; a higher percentage are males and report more oral sex partners [7].
Hypopharyngeal cancer is also one of subtype of pharyngeal malignancies whereby malignant cells grow arise from the mucosa of either one or the three anatomical subsites of the hypopharynx.The incidence of head and neck cancer has been increasing in the last few decades just as hypopharyngeal cancer cases have kept on increasing with increasing incidence in younger patients having been described in some literature [8].
Study design and participants:
This was a hospital based descriptive cross-sectional study.
It was carried out from April 2015 to December 2015 and included all patients with histological diagnosis of malignant lesions in head and neck who attended the Otorhinolaryngology MNH and Dental department at MNH in Tanzania.
Data collection and laboratory analyses:
The socio-demographic data, the clinical examination findings, Computerized Tomography (CT)/Magnetic Resonance Imaging (MRI) reports and histological results of all patients with histological diagnosis of head and neck cancer were obtained through hospital registries, computerized database and patient files.
All the information was counterchecked and corrected where necessary by using special designated coded questionnaire to interview the patient about socio-demographic data.
The clinical examination findings from the files were further discussed and reviewed by otorhinolaryngologist, head and neck surgeon then filled in special form which consisted of different head and neck anatomical sites, the CTscans/MRI were reviewed by otorhinolaryngologists,
The histology was done and reviewed by a pathologist and filled in another special form comprising of histological diagnosis.
Data analysis:
Continuous variables were summarized by medians and interquartile ranges and categorical variables were summarized by frequency and percentage. Data were analyzed using SPSS software for Windows version 16.0.
Ethical considerations:
Patients were provided with an informed consent and then asked to provide written consent to participate in the study. This study was approved by the Research and Publication Committee of the Muhimbili University of Health and Allied Sciences.
Results:
The total number of patients involved in the study with head and neck malignancies were 438.244 (55.7%) were male and 194 (44.3%) were female. Age ranged from 3 – 92 years. Those with pharyngeal malignancies were 114 (26).
|
Age |
Male |
Female |
Total |
|
0-10 years |
1(0.1%) |
0(0%) |
1(0.2) |
|
11-20years |
8(1.8%) |
4(0.9%) |
12(2.7%) |
|
21-30years |
16(3.7%) |
10(2.3%) |
26(6%) |
|
31-40years |
26(6%) |
17(3.9%) |
43(9.8) |
|
41-50years |
44(10%) |
40(9%) |
84(19%) |
|
51-60years |
64(14.6%) |
63(14%) |
127(29%) |
|
61years> |
85(19.4%) |
60(13.7%) |
154(33%) |
|
Total |
244(55.7%) |
194(44.3%) |
438(100%) |
Table 1: Demographical distribution of patients with head and neck malignancies by age and sex.
Total number of patients having pharyngeal malignancies were 114. Male were 79 (69.3%) and female were 35 (30.7%).The ratio of Male to female is 2.3 to 1. Age ranged from 11yrs to 92yrs. Majority of the patients presented at 61yrs and above as in table 2. The mean age been 55.7 and SDA is 17.6.
|
Age |
Male |
Sex |
Total |
|
11-20years |
4(3.5%) |
1(0.9%) |
5(4.4%) |
|
21-30years |
5(4.4%) |
1(0.9%) |
6(5.3%) |
|
31-40years |
10(8.8%) |
4(3.5%) |
14(12.3%) |
|
41-50years |
7(6.1%) |
6(5.3%) |
13(11.4%) |
|
51-60years |
14(12.3%) |
15(13.2%) |
29(25.4%) |
|
61years > |
39(34.2%) |
8(7.0%) |
47(41.2%) |
|
Total |
79(69.3%) |
35(30.7%) |
114(100%) |
Table 2: The distribution of patients with pharyngeal malignancies according to age and sex.
Males were more in age group above 61yrs 39(34.2%) and few in age group between 31yrs to 40yrs 4(3.5%). Most female were in age group between 51 to 60yrs 15(13.2%) and least in 11 to 20yrs been 1(0.9%)
|
Age |
Nasopharyngnx |
Oropharyngx |
Hypopharyngx |
Total |
P value |
|
n (%) |
n (%) |
n (%) |
|||
|
0-20years |
2 (40.0) |
3 (60.0) |
0 (0.0) |
5 |
0.034 |
|
21-40years |
5 (25.0) |
10(50.0) |
5 (25.0%) |
20 |
|
|
41-60years |
11 (26.2) |
20 (47.6) |
11 (26.2) |
42 |
|
|
61years> |
2 (4.25) |
30 (63.83) |
15 (31.91) |
47 |
|
|
Total |
20 (17.54) |
63 (55.26) |
31 (27.19) |
114 |
Table 3: Distribution of patient with pharyngeal malignancies according to site of occurrence by age.
There is significant difference in distribution of the pharyngeal malignancies across varies age group(p-value=0.034) Fisher`s Exact test.
Nasopharyngx occur more in the young age as compared to other malignancies;Orophanynx occurs more in the older group which is almost the same distribution with the hyopharyngeal malignancies.
|
Sex |
Site |
Total |
P value |
||
|
Nasopharyngnx |
Oropharyngnx |
Hypopharyngnx |
|||
|
n (%) |
n (%) |
n (%) |
|||
|
Male |
13(16.50) |
38(48.0) |
28(35.4) |
79(69.3) |
0.011 |
|
Female |
7(20.0) |
25(71.4) |
3(8.60) |
35(30.7) |
|
|
Total |
20(17.5%) |
63(55.3) |
31(27.2) |
114 |
|
Table 4: The distribution of patient with pharyngeal malignancies according to site by sex.
There is significant in distribution of pharyngeal malignancies between male and female with p-value of 0.011 Pearson`s chi2test
Commonly involved sites was oropharyngx (55.3%), with 48% in males and in female it was the leading part in involvement by 71.4%. In males the second most involved site was hypoharynx, by 35.4% and in females it was nasopharynx by 20%. The P value was<0.011.
|
Sex |
Histological type |
|||||||
|
SCS |
Adenocarcinoma |
Adenocystic Ca |
Lymphoma (nh) |
Kaposis sarcoma |
Undifferentiated carcinome |
Others |
Total |
|
|
Male |
63(79.7%) |
1(1.3%) |
1(1.3%) |
2(2.5%) |
6(7.6%) |
4(5.1%) |
2(2.5%) |
79(69.3%) |
|
Female |
25(71.4%) |
0(0%) |
0(0%) |
4(11.4%) |
3(8.6%) |
2(5.7%) |
1(1.9%) |
35(30.7%) |
|
Total |
88(77.2%) |
1(0.9%) |
1(0.9%) |
6(5.3%) |
9(7.9%) |
6(5.3%) |
3(2.6%) |
114(1000%) |
Table 5: The histological distribution of patients with pharyngeal malignancies by sex.
Squamous cell carcinoma was the leading histological type in both sexes. In males the second most common histological type was Kaposi’s sarcoma with by7.6% and for females was lymphoma, by11.4%. The P value was 0.56.
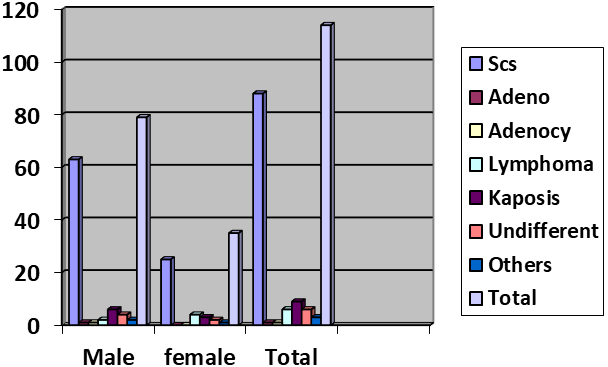
Figure 1: Show the distribution of pharyngeal malignancies histological type by sex.
Discussion:
Pharyngeal malignancy is among the most increasing cancer of Head and Neck in Tanzania and worldwide in general. The people who are commonly affected are older ones which are from 61 years and above although the trend is changing as the malignant disease is observed in young people. Patients less than 40 years were 22% involved and those above 40yrs were 78% marking the majority. Male were involved by 69.3%making the ratio of male to female been 2.3 by 1. This finding were almost the same with study done by Mwansasu et al that found 66.3% males and the rest females with a male to female ratio 2:1 were involved in the study. The mean age at the time of diagnosis was 51±18. Patients below age of 40 years accounted for 28.4% of all head and neck cancer patients and above 40year were 71.6% [2].
The prevalence of pharyngeal malignancies in this study is 26% with a mean age of 55.7 years and median age is 57.5years (SD17.63) with majority present at the age above 61years old. This is comparable to a study by Wahid et al. whom found a mean age of 57.26 years (SD 0f 14.01) with majority presenting in the 6th and 7th decade followed by those in there 4th and 5th decades.
Commonly involved site was oropharynx (55.3%) followed by hypopharynx (27.7%) and lastly nasopharynx (17.5%). In a study done in India at the Cival Hospital the commonly involved site was the oropharynx. In this study, the oropharynx cancers comprised 24.2% of all HNC and had a male to female ratio of 8:1, oral cancers comprised 23.9% and a ratio of 1:1, hypopharynx cancers comprised 18.4% and had a ratio of 8:1, larynx cancers comprised 15.6% and had a ratio of 7:1, and nasopharynx cancers comprised 5.2% with a ratio of 1:1 [10]. The finding in order of sequence is almost the same. The part of Oropharynx has been leading in female for 71.4% which is total different in literature as compared to male possibly due to increase number of oral sex,open mouth kissing, poor hygine of oral and the use of tobacco with alcohol. Also female are the ones involve in sexualy activity as part of work in our country as compared to the men.
Among the 3type of the pharyngeal malignancies nasopharyngeal malignancies is the one which occur more in the young age group with bimodal distribution.Possible this occurance is due to viral oncology and the anatomical part that is been involved which slightly is different to the other types.
The leading histological type was the squamous cell carcinoma by 77.2%, followed by kaposis sarcoma 7.9%, lymphoma 5.3%, undifferentiated carcinoma 5.3%, angiosarcoma 1.8%, adenocarcinoma 0.9%, adenocystic carcinoma 0.9%. This shows similarity in the finding when relate it with other study. With the study done by Garandawa et al. found histological prevalence of squamous cell carcinoma (73.3%), non-hodgkin’s lymphoma (13.4%), salivary malignancy (8.9%), and Kaposi”s Sarcoma (4.4%).
Conclusion and recommendation:
This study shows that the prevalence of the pharyngeal malignancies among head and neck malignancies to be 26%. The oropharynx is the most common site of the pharynx been affected with malignancies (55.3%), followed by hypopharynx (27.2%) and nasopharynx (17.5%).
Female is the most affected gender by 71.4%in the oropharynx.
Nasopharyngeal malignancies shows the distribution in young age group as compare to other pharyngeal malignancies.
The leading histological findings was the squamous cell carcinoma in all sex followed by kaposis carcoma in male and in female was lymphoma.
In this study it shows men has higher chance of acquisition of hypopharyngeal malignancies than female further studies should be done to establish the cause.
Limitation:
This is a descriptive hospital base study which covers only the patient that attended or visited the hospital ,do insist further research to be done in the community including the genetic sequencing inorder to intergrate this disease.
Declaration:
I Olivia M Kimario declare that this is my original work has not been copied nor presented to any other journal.
Study protocol was approved by the Ethics committee Muhimbili University of heathy and allied sciences with Ref no.HD/MUH/T.228/2013.
Ethical approval: Informed consent was verbal and was approved by the ethical committee. Consent for publication:
Availability of data and material: Available anytime needed.
Funding: Not applicable
Acknowledgement:
It is not possible for a single person to cover all aspects that made this article into being and therefore, at the accomplishment of this article, I would like to express my sincere gratitude to all those who helped me to reach this stage.
Competing Interest:
The authors declare no competing.
Authors` contributions:
OMK-drafting the manuscript,data collections and discussions
ER-Literature review and discussion.
FM-discussion of the manuscript and literature

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org